JINAN, China, Feb. 2, 2024 /PRNewswire/ -- On January 29th, the results of the phase II study on Qilu Pharmaceutical's novel anticancer drug iparomlimab and tuvonralimab (QL1706) were published online in Signal Transduction and Targeted Therapy (Impact Factor=39.3). The study investigated the use of QL1706 in combination with chemotherapy, with or without bevacizumab, for the treatment of non-small cell lung cancer (NSCLC). The publication of the phase II study results signifies broader recognition of QL1706 in the international clinical research community and expands the drug's impact within the global academia.
The study, led by Prof. Li Zhang from the Sun Yat-sen University Cancer Center, focused on using QL1706 in combination with chemotherapy, with or without bevacizumab, as a first-line treatment for advanced NSCLC. The research also examined the efficacy of QL1706 in combination with chemotherapy and bevacizumab in patients with epidermal growth factor receptor (EGFR)-mutant NSCLC that progressed after tyrosine kinase inhibitor (TKI) therapy. The findings indicated that QL1706, when used with chemotherapy, with or without bevacizumab, exhibited improved tolerability and promising anti-tumor activity in first-line treatment of patients with EGFR wild-type NSCLC. The combination of QL1706 with chemotherapy and bevacizumab showed notable anti-tumor effects in patients with EGFR-mutant NSCLC who did not respond to TKI therapy, presenting a potential new treatment option.
NSCLC is the predominant pathological type of lung cancer. The systemic management of advanced NSCLC has been revolutionized through advances in chemotherapy, targeted therapy, and immunotherapy, leading to extended overall survival for patients. Among immunotherapies, PD-1/PD-L1 and CTLA-4 inhibitors have become crucial in the first-line treatment of NSCLC, showing remarkable effects on survival outcomes. Despite their efficacy, these treatments can often present safety concerns. Currently, EGFR-TKIs are the standard therapy for EGFR-mutant advanced NSCLC. Despite the high initial objective response rate (ORR), tumors inevitably become resistant to first- and second-generation EGFR-TKIs. The secondary EGFR mutations are considered one possible resistance mechanism. For instance, the T790M mutation impairs binding between first-/second-generation EGFR-TKIs and mutated EGFR. Osimertinib, a third-generation EGFR-TKI, is used for treating NSCLC with EGFR T790M mutation, but its benefits in terms of overall survival are limited.
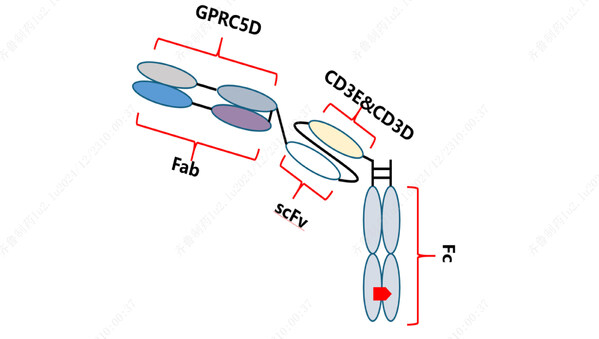
This trial was designed based on current evidence, to investigate whether dual immunotherapy plus chemotherapy (2 or 4 cycles), with or without bevacizumab, followed by maintenance therapy, could provide durable response and survival benefits. QL1706, targeting both PD-1 IgG4 and CTLA-4 IgG1, blocks both pathways. In a phase I study, QL1706 demonstrated robust anti-tumor effects in patients with advanced solid tumors, including those with NSCLC. Building on these findings, the multi-cohort phase II study assessed the effectiveness of QL1706 in combination with chemotherapy, with or without bevacizumab, in treating both EGFR wild-type and mutant advanced NSCLC. Out of the 112 patients screened in the trial, 91 were enrolled and divided into five distinct cohorts based on genotype: cohorts 1-4 comprised EGFR wild-type individuals, while cohort 5 included EGFR-mutant patients who had experienced disease progression on EGFR-TKI therapy.
The study's findings revealed that the combination of QL1706 with chemotherapy, with or without the addition of bevacizumab, demonstrated promising efficacy in the treatment of advanced NSCLC. For patients with EGFR wild-type NSCLC, the ORR was 45%, and the median progression-free survival (mPFS) was 6.8 months. Notably, the median duration of response (mDOR) was not reached, and for those who responded to the treatment, the median immune duration of response (iDOR) was 11.5 months. These outcomes provide strong support for the efficacy of QL1706. Regarding safety, grade 3 or higher treatment-related adverse events (TRAEs) were reported in 31.7% of the patients, but no grade 4 or 5 TRAEs occurred.
In patients with EGFR-mutant NSCLC that progressed after EGFR-TKI therapy, the combination of QL1706 with bevacizumab and chemotherapy resulted in an impressive ORR (54.8%) and mPFS (8.5 months). This suggests the potential advantage of the combination therapy over the use of PD-1 inhibitor combined with chemotherapy and bevacizumab. In the study, 18 (58.1%) of the EGFR-mutant patients experienced immune-related adverse events (irAEs), the most common being hypothyroidism (29%), increased aspartate transaminase (AST) level (25.8%), and increased alanine transaminase (ALT) level (22.6%). Despite the irAEs, the combination therapy was deemed safe and effective, providing a valuable treatment option for patients with EGFR-mutant NSCLC.
Link to the article:
https://www.nature.com/articles/s41392-023-01731-x